Ordinary foods, no drugs: a low-carb diet hit 62.5% diabetes remission in a 12-month RCT
A 12-month RCT in China (n=66) found that a calorie-matched low-carbohydrate diet built from ordinary foods — no shakes — achieved 62.5% T2D remission versus 35.3% on standard medication and diet advice (OR 4.59). Only 5.9% of participants dropped out. Government-funded; no conflicts of interest declared.

Research Brief
Early type 2 diabetes (T2D) remission research has a credibility problem. The trials showing the highest remission rates — DiRECT and DIADEM-I — used very-low-calorie liquid meal-replacement packs (800–853 kcal/day) dispensed by clinicians. The results were impressive. The dropout rates were also 21%, and the protocols are hard to replicate in any clinic without specialized support. Patients on ordinary diets in standard care rarely hit remission rates above 10%.
A 12-month randomized controlled trial (RCT) published in Journal of Diabetes Research on May 28, 2026, asks a more practical question: what if you simply ate less and cut carbohydrates using real food — no shakes, no meal kits — while stopping diabetes medication on day one? The answer from Wang et al. was 62.5% remission in the intervention group versus 35.3% in the energy-balanced control group. Adjusted odds ratio: 4.59 (95% CI 1.28–16.52, p = 0.020). Only 2 of 34 participants in the intervention arm dropped out. 1
What the diet actually looked like
The intervention is called CR-LCD — caloric restriction combined with low-carbohydrate diet. The name describes it exactly.
Calories were set individually, equal to each participant's basal metabolic rate (BMR) as measured by body composition analysis — not a flat 800-kcal prescription, but a personalized floor. For someone with a BMR of 1,500 kcal, that means eating roughly 1,500 kcal per day. The macronutrient split was: carbohydrates 25–30% of total energy, protein 25–35%, and fat 35–40%. 1
For a 1,500-kcal person, 25–30% carbs translates to approximately 94–113 grams of carbohydrate per day — well below a standard Chinese dietary guideline target of around 250–300 g, but above ketogenic range (<50 g). The food itself came from normal grocery sources; the trial supplied a standardized dietary guidance manual with serving-size references, common food calorie tables, and sample menus calibrated to different energy levels.
Participants followed this plan for six months. They logged meals for at least three days per week. Dietitians held two in-person sessions and four online sessions, and followed up weekly to handle problems like social dinners or flagging motivation. All diabetes medications were stopped on day one of the intervention. If fasting glucose climbed above 7 mmol/L or 2-hour postprandial glucose exceeded 10 mmol/L, or if blood sugar fell below 3.9 mmol/L, an endocrinologist stepped in. 1
The control group ate an energy-balanced diet: calories matched to BMR plus daily activity, with carbohydrates at 45–60%, protein at 15–20%, and fat at 20–35%. They received identical counseling contact hours.
Loading content card…
The trial design and who was enrolled
The study ran from June 2023 to June 2025 at the Standardized Metabolic Disease Management Center (MMC) of Ningbo No. 2 Hospital, Zhejiang Province, China. It was registered on the Chinese Clinical Trials Registry (ChiCTR2600118189) and published as an open-access article under a CC-BY 4.0 license. 1 2
129 candidates were screened; 68 were randomized 1:1 to CR-LCD or control. The enrollment criteria required: adult T2D diagnosed within the past 5 years, BMI ≥ 24 kg/m² (China's overweight threshold), and no insulin use in the past month. Anyone with a severe complication, a recent weight loss of ≥5%, or a contraindication to dietary change was excluded.
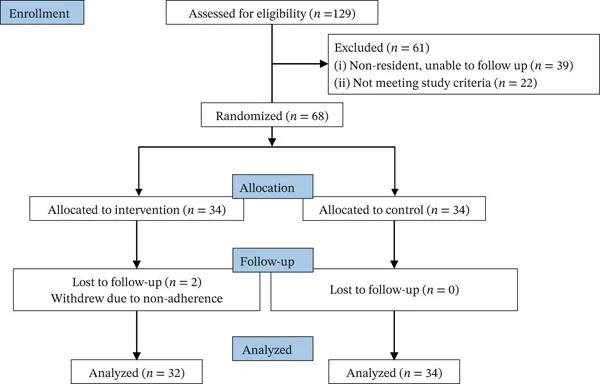
Two participants in the CR-LCD group were lost to follow-up due to non-adherence (missed meal logs and blood glucose measurements), yielding a 5.9% dropout rate and a final analyzed sample of n = 32 CR-LCD and n = 34 control. Baseline characteristics in the CR-LCD group: mean age 47.9 ± 9.8 years, 65.6% male, median T2D duration 36.5 ± 18.4 months, BMI 27.1 ± 2.6 kg/m², median HbA1c 10.05% (IQR 7.83–11.35%). One notable baseline imbalance: the control group had a significantly larger mean waist circumference (96.7 cm vs 91.5 cm, p = 0.027), which actually makes the CR-LCD result more conservative in unadjusted analyses. 1
The design is open-label: participants, dietitians, and outcome assessors were not blinded. The authors counter that the primary outcome — HbA1c < 6.5% plus off diabetes medication for ≥3 months — is an objective laboratory measure rather than a subjective rating, and that data analysis was conducted blind.
Primary result and 12-month secondary outcomes
Diabetes remission (HbA1c < 6.5% with no diabetes medication for ≥3 months): 62.5% in CR-LCD (20 of 32) versus 35.3% in control (12 of 34), χ² = 4.885, p = 0.027. After adjusting for baseline waist circumference, age, HbA1c, and T2D duration, the odds ratio was 4.59 (95% CI 1.28–16.52, p = 0.020). 1
The CR-LCD group lost a mean of 5.84 kg (75.1 → 69.2 kg, −7.8%) by 12 months; the control group showed no significant weight change. Within-group HbA1c in CR-LCD fell from a median of 10.05% to 6.30%; the control group also improved (9.90% → 6.35%) but remained on medication throughout.
Secondary outcomes reaching statistical significance at 12 months after false-discovery-rate (FDR) correction:
| Outcome | CR-LCD change | Control change | Adjusted effect size | FDR p |
|---|---|---|---|---|
| BMI | −2.02 kg/m² | minimal | η²p = 0.150 | 0.006 |
| Fasting blood glucose (FBG) | larger decrease | control FBG rose to 7.02 mmol/L | r = 0.613 | < 0.001 |
| 2-hour postprandial glucose | −1.67 mmol/L vs control | — | η²p = 0.088 | 0.040 |
| Waist circumference | −4.04 cm vs control | — | η²p = 0.085 | 0.040 |
| HDL-cholesterol | +0.197 mmol/L vs control | — | η²p = 0.095 | 0.040 |
Six-month secondary outcomes did not survive FDR correction — the metabolic signal strengthened over time, not immediately. No serious adverse events were recorded in either group: no severe hypoglycemia (symptomatic blood glucose ≤ 3.9 mmol/L) and no diabetic ketoacidosis. 1
How this compares to other T2D remission trials
The 62.5% remission rate is clinically meaningful when placed next to the existing trial landscape: 1
| Trial | Intervention | 12-month remission | Dropout rate |
|---|---|---|---|
| Wang et al. 2026 (this study) | CR-LCD from real foods, BMR calories | 62.5% | 5.9% |
| DIADEM-I (Taheri et al. 2020, Lancet Diabetes Endocrinol) | 800–820 kcal/day liquid TDR × 12 weeks | 61% | ~21% |
| DiRECT (Lean et al. 2018, Lancet) | 825–853 kcal/day liquid TDR × 12 weeks | 46% | ~21% |
| Liu et al. (Chinese multicenter RCT) | Dapagliflozin + moderate caloric restriction | 44% | not reported |
| Look AHEAD (general lifestyle) | Intensive lifestyle intervention | 9.2% at 2 years | — |
The Wang et al. remission rate matches DIADEM-I, which used a far more restrictive and harder-to-sustain liquid-formula protocol — and achieved it with a dropout rate roughly one-quarter of the comparison trial's. The authors note: "These findings suggest that compared with TDR, the CR-LCD approach may be associated with lower dropout rates and better adherence in real-world settings." 1
The CR-LCD group stopped all diabetes medications on day one; the control group remained on them throughout. The control group's HbA1c still improved to a median of 6.35% at 12 months, meaning medication — not just dietary counseling — was driving the control group's outcome. The trial is therefore a comparison of CR-LCD alone versus standard pharmacological management plus conventional diet advice, not a head-to-head dietary comparison.
Loading content card…
Limitations
The authors identified five limitations, and they are the right five to flag.
Open-label design. Participants knew which group they were in, dietitians knew, and outcome assessors knew. This introduces performance bias — people in the CR-LCD group may have been more motivated precisely because they knew they were on the "active" protocol. 1
No validated adherence measure. The trial used self-reported dietary logs, which are known to underestimate actual intake. There is no biomarker or metabolomic confirmation that participants maintained the prescribed macronutrient ratios throughout 6 months.
Single center, single population. The study took place at one hospital in eastern Zhejiang Province. The results may not transfer directly to populations with different baseline metabolic profiles, genetic backgrounds, food environments, or T2D management customs. The trial's population was predominantly male (65.6%) with relatively short T2D duration (median ~36 months) and high baseline HbA1c (~10%) — a profile that may be more responsive to dietary intervention than a general T2D clinic cohort.
Short follow-up. Twelve months is enough to confirm remission by the ADA/WHO definition (HbA1c < 6.5%, off medication ≥3 months), but it does not show whether remission persists at 2 or 5 years, or what proportion relapse.
No mechanistic measurements. The trial lacks pancreatic fat quantification, hepatic fat assessment, or indirect calorimetry — measures that would reveal whether remission was driven by caloric restriction, carbohydrate reduction, or weight loss per se. The distinction matters for protocol design but does not change the clinical finding.
Funding and conflicts of interest: The study was funded by the Zhejiang Province Medical and Health Science Research Fund (grant 2023KY1099), a regional government health research body. All authors declared no conflicts of interest. This is a meaningful difference from industry-funded dietary intervention trials; the funder had no commercial stake in the outcome. 1 2
Peer review status: Published in Journal of Diabetes Research (Wiley/Hindawi), received May 11, 2026, published May 28, 2026. Open access, CC-BY 4.0.
The recommendation
For a patient in the early stages of T2D — diagnosed within the past five years, overweight, not on insulin — this trial provides the strongest real-food evidence to date that caloric-carbohydrate restriction can achieve remission rates comparable to intensive meal-replacement protocols. The practical translation is specific:
If the goal is T2D remission rather than glycemic management on medication, the diet that produced the 62.5% result in this trial works as follows: total daily calories equal to individually measured BMR (not a flat budget), with carbohydrates holding to 25–30% of energy (roughly 90–115 g/day for most adults), protein at 25–35%, and fat at 35–40%. The food comes from normal grocery sources, structured around a standardized guide that assigns portions to common foods. The protocol requires stopping diabetes medication on day one, which mandates close medical supervision and a reliable blood glucose monitoring plan.
For a dietitian advising this population, the practical implication is different from the headline number. The 62.5% rate applies to a carefully selected group: early-stage T2D (under 5 years since diagnosis), overweight but not severely obese, insulin-naive, and enrolled in a structured program with six months of weekly dietitian contact. A patient on insulin, with a decade of T2D history, or without access to regular dietary counseling is not the population this trial describes, and the remission estimate should not be extended to them.
The drug-free remission at 12 months — confirmed by an objective HbA1c threshold — and the absence of serious adverse events are the trial's strongest signals. The single-center, open-label design and lack of long-term follow-up are genuine constraints. Independent replication in a broader population, with objective adherence measures, is the logical next step before this protocol moves into routine clinical guidance.
Cover image: AI-generated illustration.
Add more perspectives or context around this Post.